General
- sulfonamides are antifolate drugs
- basic formula --> similar to p-aminobenzoic acid (PABA)
- some microbes require extracellular PABA to form dihydrofolic acid --> form purine and nucleic acid
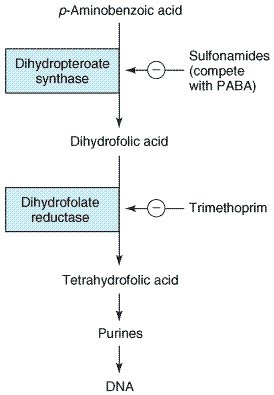
- mechanism of action - competitively competes with PABA as above
- susceptibility: g+ve, g-ve, nocardia, chlamydia, protozoa, some enteric bacteria (e coli, klebsiella, salmonella, shigella, enterobacter)
- rickettsia NOT inhibited by sulfonamides - stimulated by it
Resistance
- some bac dont have enzymes for folate systhesis - nothing to block
- overproduction of PABA due to mutation
- production of enzyme that has low affinity to sulfonamides
Pharmacokinetics
- po/iv - metabolised by liver --> urinary excretion *reduce dose for renal pt
Clinical uses
- hardly used anymore alone
- needs combination
TRIMETHOPRIM
- inhibits bacterial dihydrofolic acid reductase --> see diagram
- binds 50,000 times more efficiently than same enzyme
- creates synergism with sulfanamides
- combination is bactericidal vs bacteriostatic alone
Resistance - due to plasmid encoded mutation
- reduced cell permeability
- overproduction of dihydrofolate reductase
- mutation of reductase - reduced drug binding
Pharmacokinetics
- po or iv
- absorbed well orally
- 1:5 preparation with sulfamethoxazole - peak concentration in serum 1:20 (due to increased lipid solubility)
- concentrates in prostatic fluid and vaginal fluid (more acidic) --> more antibacterial activity
- renal excretion
Uses
- UTI - prostatitis
- PCP
- GIT - shigellosis, salmonella infection
- respi - strep pneumoniae, haemophilus, M catarrhalis, K pneumoniae
- not mycoplasma
SE
- antifolate --> megaloplastic anemia, bone marrow suppresion
- can give folinic acid for prevention
No comments:
Post a Comment